Orbital cellulitis
- patient: patients with siniusitis. Children.
- pathophysiology: infection of fat and extraocular muscles of eyes
- viridans strep, strep pneumo, staph aureus
- Sx:
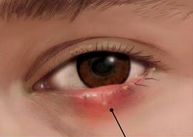
- erythema, edema, and tenderness, often with impaired extraocular movement.
- Only orbital cellulitis involves the post-septal (ie, orbital) structures such as the extraocular muscles (ophthalmoplegia, painful eye movements) and orbital fat (proptosis).
- Dx: CT or MRI scan, look for abscess/purulence
- Rx: empiric IV abx third-generation cephalosporin (eg, ceftriaxone) or ampicillin-sulbactam (covers strep pneumo, viridans, H flu, staph aureus. For patients with a history of methicillin-resistant S aureus or whose clinical presentation is severe, vancomycin should be added.
- Surgery for abscess
Orbital cellulitis is more concerning and can be differentiated from the less serious, but more common, preseptal cellulitis by identifying signs or symptoms suggestive of intra-orbital inflammation.

Preseptal cellulitis
- patient:
- pathophysiology: Preseptal cellulitis may be secondary to sinusitis but more commonly is due to breaks in the skin. As a result, S aureus and S pyogenes are common causes of preseptal cellulitis.
- Sx: no painful eye movement
- Rx: oral abx